Tinnitus After 60: Causes of Louder Ringing and Effective Treatments
Introduction — Why tinnitus often feels louder after 60
If you’ve noticed tinnitus after 60—ringing, buzzing, hissing, or other sounds that seem to come from inside your ears—you’re far from alone. Tinnitus is common, and while it can be frustrating (especially at night), it’s often manageable with the right plan.
So why can it feel like it suddenly got louder now? In many older adults, tinnitus becomes more noticeable because of overlapping factors: age-related hearing changes (presbycusis), the brain’s compensation process (turning up gain), hormonal and neurochemical shifts with aging, and side effects from certain medications. The encouraging news: many people experience improvement in tinnitus distress or loudness with hearing-focused solutions and therapy-based strategies (Mayo Clinic).
A simple way to think about it: tinnitus doesn’t always increase—sometimes the environment gets quieter (retirement, fewer noisy workplaces, fewer social gatherings), hearing changes make outside sound less crisp, and the brain pays more attention to the internal signal. As one clinician might put it: When speech gets harder to hear, the brain starts listening harder to everything—including tinnitus.
Conclusion: Many people notice tinnitus more after 60 because hearing changes and quieter environments make the internal sound more noticeable—and help is available.
What tinnitus is (and what it isn’t)
Tinnitus can sound different from person to person and may be in one ear or both, intermittent or constant. Some people notice it most in quiet environments—like when trying to fall asleep or when they wake up at 3 a.m. (Mayo Clinic).
Practical tip: Note which ear, whether it’s high or low pitched, and whether it changes with stress, caffeine, or sleep. These details help clinicians narrow likely contributors.
Common tinnitus sounds people describe after 60
- Ringing
- Buzzing
- Hissing
- Roaring
- Clicking
Tinnitus is a symptom, not a disease
Tinnitus isn’t a single diagnosis—it’s a symptom reflecting changes in hearing pathways or an underlying ear/health condition. The best approach: identify contributors, support hearing and the auditory system, and reduce the distress and attention the sound can trigger (American Tinnitus Association). Think of tinnitus like a check engine light—it signals something needs a closer look.
Conclusion: Naming what you hear and when it changes can speed up the path to tailored care.

Symptoms checklist — when tinnitus after 60 is expected vs. a red flag
Typical tinnitus symptoms in older adults often include:
- More noticeable in quiet rooms or at bedtime
- Often paired with hearing difficulty (understanding speech in noise, missing consonants)
- Stress, fatigue, and poor sleep can make it feel louder or more intrusive
This doesn’t mean it’s all in your head—your brain and nervous system influence how strongly tinnitus stands out. The spotlight analogy fits: the more you scan for the sound, the brighter it can feel (Harvard Health).
Red flags — seek urgent or prompt care if you have:
- Sudden hearing loss (same day or within ~72 hours)
- New tinnitus in one ear only, especially with hearing change
See: https://sleepandsinuscenters.com/blog/single-sided-tinnitus-when-to-seek-urgent-medical-attention
- Pulsatile tinnitus (a heartbeat or whooshing sound)
See: https://sleepandsinuscenters.com/blog/pulsatile-tinnitus-red-flags-key-symptoms-to-watch-for
- Severe dizziness/vertigo, facial weakness, or other neurological symptoms
- Ear pain, drainage, fever, or rapidly worsening symptoms
These symptoms don’t always mean something serious, but they do warrant prompt medical evaluation (Mayo Clinic).
Conclusion: If your pattern fits the typical profile, start with hearing and lifestyle support; if red flags are present, seek prompt care.

Why tinnitus often worsens after 60 (the brain + ear explanation)
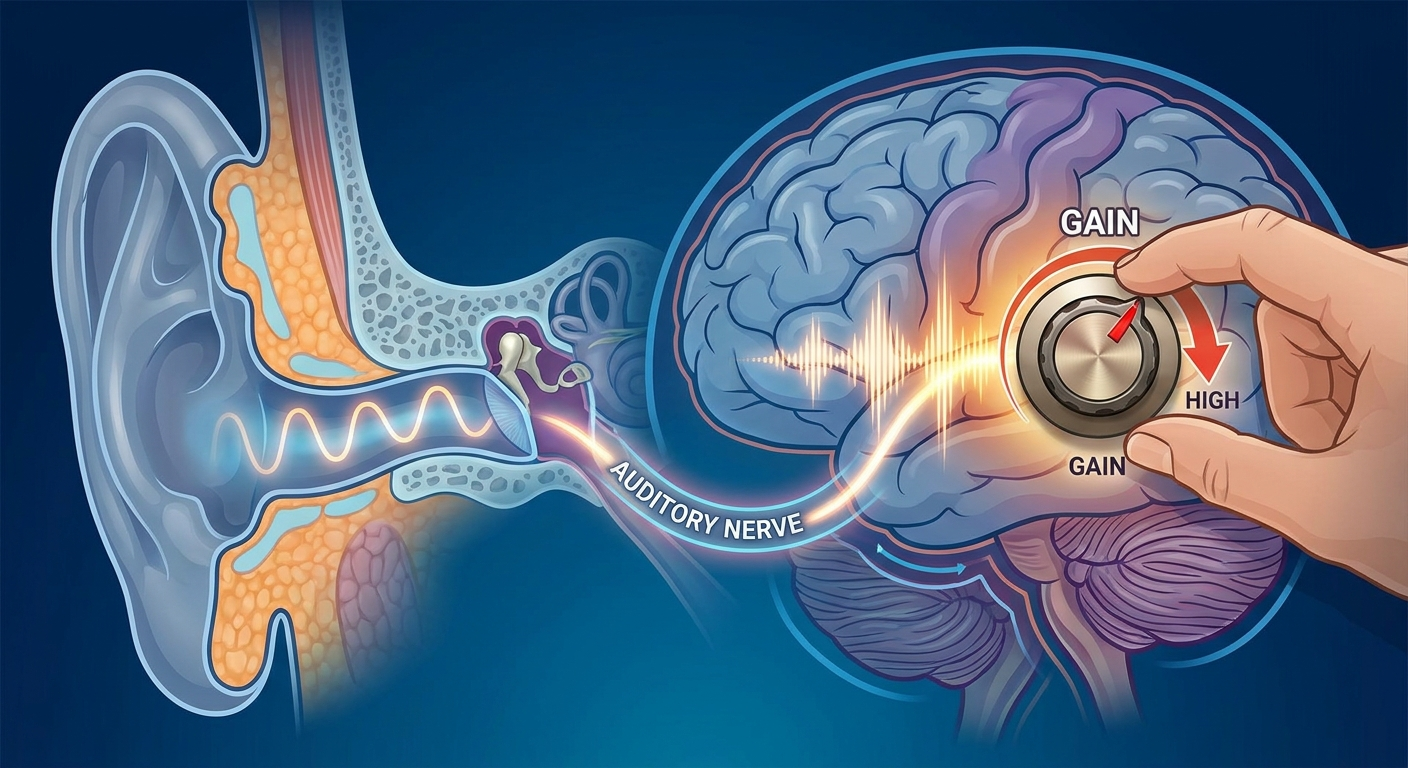
Presbycusis (age-related hearing loss) is a common driver. As inner ear hair cells and auditory pathways decline, the brain receives less sound and may fill in gaps, increasing tinnitus perception (Mayo Clinic). Many people report relief with hearing aids because amplification restores missing external sound and reduces contrast (NCOA). If you’re turning up the TV or asking for repeats—especially in restaurants—tinnitus can become the default background your system locks onto.
The brain turns up the volume (increased auditory gain). Like a radio with weak reception, when input is low, the system raises sensitivity. Tinnitus often seems worst in silence (bedtime) because there’s less real-world sound to compete. Many describe: Once the room goes quiet, the ringing steps forward (Harvard Health).
Conclusion: When the ears provide less input, the brain often listens harder—especially in quiet.
Causes and risk factors of louder tinnitus in seniors (most common to less common)
Hearing loss + sound deprivation (most common)
- Presbycusis plus lower day-to-day sound input lets tinnitus stand out. Past noise exposure can contribute, even decades later (Mayo Clinic; ATA).
Medication-related tinnitus (ototoxicity)
- Categories clinicians may review include loop diuretics, certain antibiotics, some chemotherapy agents, and high-dose salicylates/NSAIDs. Do not stop medications abruptly; discuss timing of changes with a clinician (Mayo Clinic).
Hormonal and neurochemical changes with aging
- Age-related shifts, including menopause-related estrogen decline in some individuals, may play a role (PMC reviews).
Ear conditions that can amplify perception
- Earwax buildup
- Middle ear fluid/Eustachian tube dysfunction
- Ear infections or inflammation
Learn more about earwax: https://sleepandsinuscenters.com/blog/earwax-impaction-symptoms-and-effective-removal-tips (Mayo Clinic).
Health conditions that can worsen tinnitus
- High blood pressure/vascular disease (especially if pulsatile)
- Diabetes and circulation changes
- TMJ/clenching
- Anxiety/depression and chronic stress
Conclusion: Several small factors often add up; addressing the fixable ones can make a big difference.
How doctors evaluate tinnitus after 60 (what to expect at an ENT/audiology visit)
Key history questions
- When did it start? Is it getting worse?
- One ear or both? Pulsatile or non-pulsatile?
- Any hearing difficulty or noise exposure?
- Full medication list (including OTCs and supplements)
Deeper overview: https://sleepandsinuscenters.com/blog/ent-care-for-tinnitus-relief-effective-treatments-and-tips
Tip: Bring a brief timeline, e.g., Noticed ringing in March; worsened after a medication change in April; worst at night; no dizziness.
Exam and testing
- Ear exam (wax, infection, eardrum)
- Audiogram (hearing test), sometimes speech-in-noise
Guide: https://sleepandsinuscenters.com/blog/audiogram-basics-explained-a-patients-guide-to-hearing-tests
When imaging or specialty testing is needed
- Considered for pulsatile tinnitus, clearly one-sided tinnitus with asymmetric hearing, or neurological symptoms (Mayo Clinic).
Conclusion: A clear history, ear exam, and hearing test usually provide the roadmap for next steps.
Most effective treatments for tinnitus after 60 (evidence-based, practical)
Top option when hearing loss is present: hearing aids
- Improve access to everyday sounds
- Reduce contrast with tinnitus
- Ease communication and stress
Ask your audiologist: built-in tinnitus programs, open vs. closed fit, and follow-up schedule (NCOA).
Sound therapy and masking strategies (especially for nighttime)
- White noise or nature sounds
- Fan or air purifier
- Bedside speaker or sound pillow
- Apps or dedicated sound generators
Principle: blend, don’t blast. Step-by-step tips: https://sleepandsinuscenters.com/patient-resources/masking-technique-tinnitus (Mayo Clinic).
CBT (Cognitive Behavioral Therapy)
- Reduces distress and hypervigilance even if sound remains (Mayo Clinic; ATA).
TRT (Tinnitus Retraining Therapy)
- Counseling plus sound strategies to reclassify tinnitus as unimportant background; can combine with CBT (PMC reviews).
Treat the underlying trigger when present
- Safe in-office wax removal
- Treat middle-ear fluid/infection when diagnosed
- Address TMJ/clenching (night guard, PT, dental care)
- Support vascular contributors (especially with pulsatile patterns) (Mayo Clinic)
What to be cautious about
- Online cure supplements (limited evidence; interactions possible)
- Overusing earbuds at high volume
- Stopping prescriptions abruptly without review (ATA)
Conclusion: Support your hearing, lower the contrast, and retrain attention—these pillars help many people feel better.

Lifestyle tips for long-term relief (especially helpful after 60)
Hearing protection—without over-protecting
- Use protection in truly loud settings; avoid constant silence. Keep normal daily sound in your life so tinnitus has less contrast (ATA).
Sleep strategies for tinnitus
- Sound enrichment at bedtime
- Consistent sleep schedule
- Reduce monitoring the sound; consider CBT-I if insomnia is significant
Stress, mood, and attention management
- Exercise, gentle breathing, social engagement, and mindfulness reduce the alarm response (Harvard Health).
Medication review checklist
- Note start dates near tinnitus changes
- List OTCs (NSAIDs, cold meds, sleep aids)
- Ask about alternatives based on your health profile (Mayo Clinic)
Conclusion: Consistent, gentle habits calm the nervous system and make tinnitus easier to live with.
FAQs
Why is my tinnitus louder at night?
- Less external sound means tinnitus has less competition; brain gain, stress, and fatigue can also increase intrusiveness (Harvard Health).
Can tinnitus after 60 be cured?
- Often not cured, but frequently becomes less bothersome with hearing support, sound strategies, CBT, and TRT—especially when contributors are addressed (Mayo Clinic).
Do hearing aids really help tinnitus?
- For people with hearing loss, amplification improves access to sound and reduces contrast; many report meaningful relief (NCOA).
What medications can worsen tinnitus in older adults?
- Some diuretics, certain antibiotics, and other ototoxic drugs can contribute in susceptible individuals or at certain doses (Mayo Clinic).
Should I see an ENT or an audiologist first?
- New, one-sided, pulsatile tinnitus, or tinnitus with dizziness/neurological symptoms: start with ENT. Longstanding tinnitus with gradual hearing difficulty: audiology testing is a key first step; ENT as needed (Mayo Clinic).
Conclusion: With the right plan, most people find tinnitus becomes less intrusive over time.
When to book an appointment
Consider scheduling an evaluation at Sleep and Sinus Centers of Georgia if tinnitus after 60 is new or worsening, affecting sleep/mood/concentration/hearing, or is unilateral or pulsatile.
Request a tinnitus-focused visit or hearing evaluation: https://www.sleepandsinuscenters.com/appointments

Sources
- Mayo Clinic. Tinnitus: Symptoms & causes. https://www.mayoclinic.org/diseases-conditions/tinnitus/symptoms-causes/syc-20350156
- Mayo Clinic. Tinnitus: Diagnosis & treatment. https://www.mayoclinic.org/diseases-conditions/tinnitus/diagnosis-treatment/drc-20350162
- American Tinnitus Association (ATA). Causes of tinnitus. https://www.ata.org/about-tinnitus/why-are-my-ears-ringing/causes/
- National Council on Aging (NCOA). Do hearing aids help tinnitus? https://www.ncoa.org/article/do-hearing-aids-help-tinnitus/
- Harvard Health. Why is the ringing in my ears getting worse? https://www.health.harvard.edu/diseases-and-conditions/why-is-the-ringing-in-my-ears-getting-worse
- PubMed Central (PMC) review example: https://pmc.ncbi.nlm.nih.gov/articles/PMC9761006/
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.